|
|

|

|
|
|
Acupuncture, Opioid Prevention, and Medicaid PolicyClaims data and practical Medicaid studies show a clear policy lesson: good policy supporting real access to acupuncture can reduce pain, improve function, reduce opioid exposure, and save lives. Bad policy can make acupuncture coverage so limited, fragmented, or difficult to use that its public-health value is never realized. 1. Direct access and opioid prevention: OptumLabs / BMJ Open claims data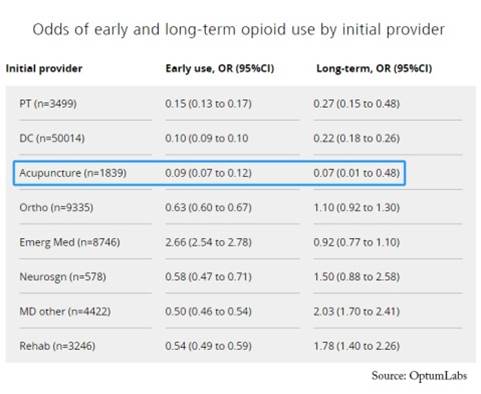
The odds of early opioid use for those who saw a physical therapist first were 85% lower than those who saw a PCP first. The odds of early opioid use were even lower for those seeing a chiropractor and acupuncturist (90% and 91%, respectively). This evidence is especially useful because it is practical and outcome-based. It does not merely ask whether acupuncture can reduce pain in a controlled setting. It asks what happens in the real healthcare system when patients with new-onset low back pain enter care through different first-contact providers. The policy implication is that direct access to licensed acupuncturists may help prevent patients from entering an opioid-centered pathway in the first place. Study link: Observational retrospective study of the association of initial healthcare provider for new-onset low back pain with early and long-term opioid use, BMJ Open, 2019. DOI: 10.1136/bmjopen-2018-028633. 2. A Medicaid model demonstrating value: Vermont pragmatic acupuncture studyThe Vermont Medicaid study is a strong example of what can happen when acupuncture is treated as a real course of care rather than a token benefit. The 2016 Vermont legislature commissioned a pragmatic study of acupuncture for chronic pain in the Medicaid population. A total of 156 Medicaid patients with chronic pain were offered up to 12 acupuncture treatments within 60 days, delivered in the offices of 28 Vermont licensed acupuncturists. Patients received an average of 8.2 treatments and showed significant improvements in pain intensity, pain interference, physical function, fatigue, anxiety, depression, sleep disturbance, and social isolation. Among patients using opioid medication, 32% reported reduced opioid use after the intervention. Among employed patients, 74% reported improved capacity to work. This is useful policy evidence because it shows the benefits of an LAC-designed, LAC-delivered intervention: decreased pain, reduced medication use, improved quality of life, and better functional outcomes. Study link: Acupuncture for Chronic Pain in the Vermont Medicaid Population: A Prospective, Pragmatic Intervention Trial, Global Advances in Health and Medicine, 2018. DOI: 10.1177/2164956118769557. Free full text: PMC5896847. 3. A Medicaid model without value: Minnesota DHS claims-data studyIn contrast, Minnesota DHS issued a report in 2018 from a retrospective claims-data study of patients using acupuncture under MN’s MHCP acupuncture policy. This policy uses confusing language and nonstandard criteria and limitations, such as measuring acupuncture in units rather than visits. Where Medicare sets a standard of 12 visits consisting of 3 units each before requiring documented progress for authorization, MN MHCP says: “up to 20 units of acupuncture services,” equating to 6 visits, before requiring documented progress. It further bundles all time and non-time based services including assessments within acupuncture time without clear guidance. As a result, DHS found that the median MHCP acupuncture user had only 4 distinct treatment days, while the average was 6.3. DHS then defined 6 or more treatment days as the threshold for having received acupuncture as a “treatment.” This demonstrates that the average patient barely reached the minimum treatment threshold, while the median patient did not reach it at all. And the study found no statistically significant reduction in later opioid use. The report acknowledges that Minnesota's Medicaid structure did not reliably keep patients engaged in care long enough to test acupuncture's value. Minnesota's model illustrates the problem with limited and unclear policies: if the service is limited, difficult to access, and unclear, the healthcare system will see no meaningful benefits. Report link: Minnesota Department of Human Services acupuncture and opioid-use claims-data report Bottom lineThe evidence supports practical, LAC designed polices. Rather than being covered only as a narrow procedure after conventional care has failed it, acupuncture should be supported as a direct-access, first-contact, nonopioid care option for appropriate pain conditions, with enough visits and administrative simplicity to allow patients to engage in a real course of treatment. |
|
|
|